
A hospital CTO usually doesn't call a meeting because software delivery is going well. The meeting happens when a patient portal release slipped again, a telehealth integration broke in staging, or security raised a blocker days before go-live. Everyone agrees the current process is too manual. No one agrees on what to change first.
That's where DevOps in healthcare stops being a tooling conversation and becomes an operating model. If your teams need to ship updates to clinician workflows, patient-facing apps, analytics services, and AI features without creating compliance risk, you need a delivery system that is repeatable, auditable, and resilient under pressure. The same foundation that helps teams release safely also becomes the prerequisite for modern AI governance, especially when prompts, models, and data flows start changing faster than traditional release processes can handle.
Why DevOps Matters Now in Healthcare
Healthcare software used to tolerate slow change. That's no longer true. Patient portals, scheduling systems, remote care workflows, billing integrations, and internal clinical tools all sit much closer to the care experience than they did a few years ago. When release cycles drag, the business impact shows up fast. Support queues grow, clinicians work around broken workflows, and security teams inherit rushed last-minute reviews.
This is why DevOps matters now. It gives healthcare organizations a disciplined way to move from fragile, manual releases to controlled delivery with built-in testing, versioning, and operational visibility. A 2021 Redgate Software report found that 73% of global IT professionals in healthcare had adopted DevOps, which shows the practice had already moved into the mainstream of healthcare IT by the early 2020s, according to Bekey's summary of the report.
What changed
Three realities pushed DevOps from “nice to have” into core infrastructure:
- Software became operationally critical. Patient access and clinician productivity now depend on digital systems behaving predictably.
- Compliance got closer to engineering. Auditability, access controls, and release traceability can't wait for a quarterly review.
- AI modernization raised the bar. Teams adding recommendation engines, summarization, triage support, or document extraction need stronger delivery controls, not weaker ones.
A lot of executives still hear “DevOps” and picture a faster deployment pipeline. That's too narrow. In healthcare, a key value is that DevOps creates a reliable system for change. It lets engineering, operations, and security work from the same set of controls instead of handing risk back and forth.
Practical rule: If your release process depends on tribal knowledge, a single hero engineer, or a freeze window that everyone fears, you don't have a scaling problem. You have an operating model problem.
The organizations making real progress don't treat DevOps as a side project for the platform team. They treat it as the mechanism that lets digital health products evolve without putting uptime, compliance, or patient trust at risk.
Defining DevOps in a Healthcare Context
A hospital rolls out a patient messaging update on Thursday afternoon. By Friday morning, appointment reminders are delayed, the contact center is flooded, and no one can say with confidence which config changed, who approved it, or how to roll it back. In healthcare, that is not a minor release problem. It is an operating model failure.
DevOps in healthcare is the discipline of making software change controlled, traceable, and repeatable across clinical and business systems. It applies to the code, the infrastructure, the approvals, and the feedback loop after release. That matters in environments where one product may depend on identity services, EHR integrations, payer workflows, patient communications, and analytics pipelines at the same time.
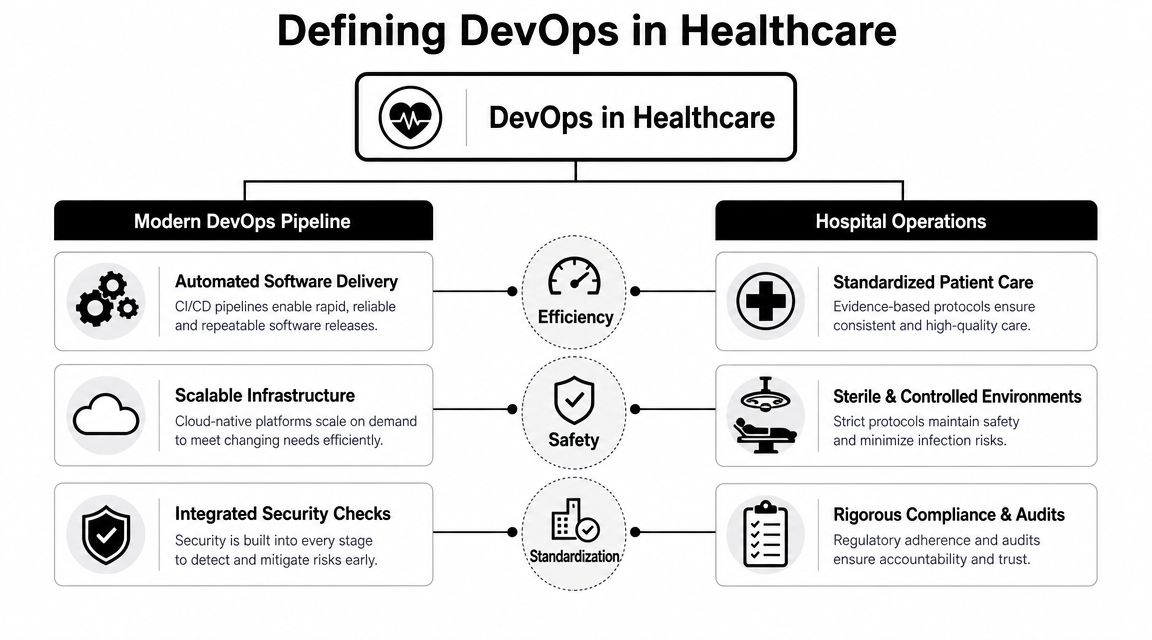
The healthcare-specific difference is accountability. In a mature DevOps model, engineering, operations, QA, security, and product work from the same delivery system and the same definition of production readiness. Release decisions are based on test evidence, environment parity, monitoring coverage, rollback plans, and access controls, not on whether the right person happens to be online.
Culture comes first because handoffs create blind spots. If developers are measured only on shipping features, operations is measured only on uptime, and security arrives at the end, the organization gets delay, rework, and arguments over ownership. Teams perform better when the people building the change also have visibility into deployability, supportability, and downstream risk.
That point matters even more for AI and ML work. A model update, prompt change, feature flag, or data pipeline adjustment can alter behavior in ways that are harder to spot than a broken button. Healthcare organizations adding ambient documentation, prior auth automation, triage support, or clinical summarization need DevOps because they need disciplined release mechanics for probabilistic systems, not just web apps.
The practical building blocks
The underlying practices are familiar, but the bar is higher in healthcare because failures hit operations fast.
| Pillar | What it means in healthcare |
|---|---|
| Continuous integration | Code is merged frequently, tested early, and validated against the integrations that matter to care and revenue operations |
| Continuous delivery | Every release candidate follows the same path to production, with approval evidence and rollback steps already defined |
| Infrastructure as code | Environments are declared in version control so configuration drift is visible and recoverable |
| Monitoring and observability | Teams can see failures, latency changes, interface issues, and unusual system behavior before clinicians or patients report them |
In practice, that means standardized environments, role-based access, controlled secrets, automated tests in pull requests, and deployment workflows that can be audited. Teams that want a stronger security foundation in DevOps pipelines usually start by reducing manual steps, because manual steps are where undocumented exceptions and inconsistent controls tend to appear.
For organizations already managing Azure DevOps for CI/CD, the same principle applies. The tooling matters less than whether repositories, pipelines, approvals, and environment definitions are managed as part of one operating system for delivery.
In healthcare, "it worked on my machine" means your release process still depends on luck.
Containers, CI/CD, and infrastructure as code are useful because they preserve consistency between environments and make change history visible. That gives teams a stable base for modernizing patient-facing products and for introducing AI features that need tighter validation, safer rollout patterns, and clearer operational ownership.
A good shorthand is this: DevOps is how healthcare organizations turn software delivery from a series of risky events into a managed clinical-grade process.
Embedding Security and Compliance by Design
Security reviews at the end of a release cycle don't work in healthcare. By that point, the architecture is set, the deadlines are fixed, and the team is negotiating exceptions instead of reducing risk. DevSecOps fixes that by moving security and compliance controls into the delivery pipeline itself.

Healthcare DevOps guidance consistently recommends encryption at rest and in transit, data masking in non-production environments, vulnerability scanning, and automated compliance checks because patient data is sensitive and auditability is mandatory. It also points out the technical cause and effect: masking and secret management reduce exposure during test and QA, while policy-as-code and infrastructure-as-code create an immutable change trail that supports HIPAA- and GDPR-aligned controls and incident response, as outlined in Gart Solutions' healthcare DevOps guidance.
What good DevSecOps actually looks like
The strongest healthcare teams don't bolt security onto releases. They build a pipeline where unsafe changes are hard to merge in the first place.
- Data protection in lower environments: Test and QA systems should use masked data, not convenient copies of production records.
- Centralized secrets handling: Credentials shouldn't live in repos, shared documents, or deployment scripts.
- Automated policy enforcement: Security gates should run the same way every time, not depend on who happens to be reviewing.
- Traceable infrastructure changes: Teams should be able to answer who changed what, when, and why without reconstructing events from memory.
For teams standardizing their Microsoft stack, this guide to managing Azure DevOps for CI/CD is a useful operational reference because it maps repository and pipeline discipline to day-to-day release work instead of treating governance as an abstract policy problem.
Speed without control is just a faster failure mode
A common misconception is that DevOps pushes teams to release recklessly. In healthcare, mature DevOps does the opposite. It narrows the path to production so that every approved release passes through the same security and compliance checks.
That's where policy-as-code becomes powerful. Instead of relying on a reviewer to remember whether an environment meets the right control set, the pipeline enforces the rule automatically. Instead of manually checking whether encryption is configured correctly, teams validate it in the build and deployment path. For a deeper look at practical controls, this overview of security in DevOps is a helpful companion read.
Security maturity in healthcare isn't about saying “no” more often. It's about making the safe path the default path.
The trade-off isn't speed versus safety. It's manual ambiguity versus automated control. Healthcare organizations that understand that tend to release with less friction and fewer unpleasant audit surprises.
Building a Compliant Healthtech CI/CD Pipeline
A release is approved at 4:30 p.m. for a patient scheduling update. By 6:00 p.m., the team learns the deployment changed an API contract, broke an intake workflow, and triggered a permissions issue in staging that never showed up earlier because staging did not match production. In healthcare, that is not a minor process miss. It is an operational failure with patient, compliance, and revenue consequences.
A compliant pipeline prevents that class of failure by making every change travel through the same controlled path. The goal is not flashy automation. The goal is repeatability, traceability, and fast rejection of unsafe changes before they reach production.
Healthcare teams feel this pressure more than most because a single release often touches patient apps, clinician workflows, payer integrations, identity systems, and data exchange services at the same time. A good pipeline gives engineering, security, and compliance teams one shared release mechanism with clear evidence at each gate. That operating model also matters for AI readiness. Once teams start shipping model-backed features, summarization, or decision support, they need the same discipline for prompts, model configs, connectors, and rollback plans that they already apply to application code.
A practical release path
The strongest healthtech pipelines are opinionated. They remove discretionary steps and make risky behavior difficult.
- Code enters through pull requests with structured review. Review criteria should cover integration impact, access control changes, and data handling, not just code quality.
- Builds run in a clean, reproducible environment. If a service only builds on one engineer's laptop, it is not ready for regulated production.
- Automated tests run by layer. Unit tests catch local logic defects. Integration and contract tests catch failures in EHR interfaces, scheduling services, identity providers, and other external dependencies.
- Security checks run in the same pipeline, not in a separate spreadsheet-driven process. Secret scanning, dependency review, container scanning, and deployment policy validation should happen before release approval.
- Staging mirrors production closely enough to expose real risk. That includes configuration, network rules, service dependencies, and role mappings.
- Production releases happen with rollback, logging, and alerting already defined. A deployment without live observability is an experiment on a clinical system.
That discipline scales better than heroics. Teams spend less time chasing one-off release errors and more time improving patient and staff experiences.
Where pipelines usually fail
The common problem is partial automation. Teams automate the clean path, then rely on tribal knowledge for the dangerous parts.
Typical weak spots include:
- Staging differs from production. Configuration drift hides failures until the release is already in motion.
- Integration coverage is thin. The application passes tests, but referral sync, eligibility checks, or document exchange breaks after deployment.
- Secrets are handled inconsistently. One service pulls from a managed vault. Another still depends on a manually updated config file.
- Approvals are documented, but not enforced in tooling. Auditors get screenshots instead of durable release evidence.
- Monitoring starts after go-live. The team finds out from support tickets instead of telemetry.
Containerization often helps because it reduces environment drift and standardizes packaging. Kubernetes can be the right choice for multi-service platforms, but it should solve a specific scaling or orchestration problem. It is not the starting point. I usually advise hospital and digital health teams to get image standards, environment configuration, release approvals, and observability under control first. That foundation produces better results than adopting more platform complexity too early.
One more point gets missed in boardroom discussions. Pipeline quality affects business operations outside engineering. If a release process causes recurring defects in eligibility, coding, claims, or patient billing workflows, the downstream cost is real. Process automation in revenue operations can help organizations cut denials and speed cash flow, but those gains are easier to sustain when the software delivery path itself is stable and auditable.
Teams that need a practical reference can use this guide to CI/CD pipeline best practices for growing engineering teams to pressure-test how they handle build consistency, approvals, testing depth, and maintainability over time.
Powering AI Modernization with DevOps
Healthcare leaders often talk about AI as if it's a separate initiative from application delivery. It isn't. If your organization can't safely version APIs, trace changes across environments, govern access to sensitive data, and observe behavior after release, you're not ready for production AI.
That's why DevOps in healthcare has become the foundation for AI modernization. Once teams add model-driven features, retrieval workflows, clinical summarization, coding assistance, or operational automation, the release problem gets harder. You're no longer shipping only application code. You're shipping prompts, model configurations, policy rules, connectors, and data-dependent behavior.
From DevOps to controlled automation
Healthcare-focused guidance notes a key challenge here: teams need to operationalize continuous security, auditability, and policy enforcement when AI models, APIs, and data flows change rapidly. The stronger emerging view is that healthcare DevOps is moving from generic automation to controlled automation, meaning continuous compliance, immutable infrastructure, and embedded security checks in every release, as described in KMS Technology's analysis of DevOps in healthcare.
That phrase matters. Controlled automation is the difference between an AI feature that looks impressive in a demo and one that survives risk review, production monitoring, and regulatory scrutiny.
What AI changes operationally
AI introduces a different kind of release management challenge:
| AI delivery concern | Why DevOps discipline matters |
|---|---|
| Rapidly changing prompts and parameters | Teams need versioning and rollback, not ad hoc edits |
| Model and API dependency changes | Security checks and compatibility testing need to happen continuously |
| Sensitive data movement | Access control, encryption, and logging must follow the workflow end to end |
| Business-critical automation | Observability has to show not only uptime, but behavior quality and failure paths |
This is especially relevant for revenue-cycle and operational workflows. If you're looking at where automation can directly improve downstream financial operations, this piece on how to cut denials and speed cash flow is a practical example of the business case leaders are trying to support with better delivery discipline.
AI programs stall when leaders treat governance as paperwork. In reality, governance is a product capability. Teams need release controls that can track what changed, who approved it, what data it touched, and how to revert it safely. That's one reason healthcare organizations exploring intelligent products should also think in terms of delivery foundations, not just model selection. This guide to AI solutions for healthcare is useful for connecting those technical decisions to real product use cases.
Your Roadmap for DevOps Adoption
DevOps adoption fails when leaders try to “transform everything” at once. The better approach is narrower and more disciplined. Start with one service that matters, one team that can own the outcome, and one release process you can make visibly better.
Start with a pilot that has real operational consequences
Pick a system that people care about. A patient scheduling component, intake workflow, integration layer, or internal clinician tool works better than a low-stakes sandbox because the lessons are real. The pilot should include development, operations, security, and whoever owns service reliability after release.
Focus on a few concrete changes:
- Move deployments into a repeatable pipeline: Every release should follow the same path.
- Version the infrastructure: If environments are still hand-built, fix that early.
- Automate test gates: Pull requests need more than human optimism.
- Define rollback before release: If the team can't explain recovery, the release isn't ready.
Build the team model, not just the toolchain
A hospital CTO doesn't need every developer to become an SRE. But the organization does need clearer ownership.
A workable structure usually includes product-aligned engineering teams that can ship independently, plus a platform function that standardizes pipelines, secrets, observability, and environment management. Security should participate early enough to shape controls, not just reject them at the end. Clinical and compliance stakeholders don't need to review every line of code, but they should influence acceptance criteria for risk-sensitive workflows.
Mature DevOps in healthcare shows up in behavior. Teams ask how a release fails, how it rolls back, and how it gets audited before they ask how fast they can ship it.
Treat resilience as part of delivery
One of the most overlooked questions in healthcare DevOps is how teams prove recoverability when clinical systems fail. Healthcare-focused guidance argues that DevOps platforms need immutable backups and a recovery plan to protect HIPAA, GDPR, and HITECH obligations and to keep care running after outages or attacks, as discussed in GitProtect's article on healthcare backup and disaster recovery strategy.
That means your roadmap should include more than CI/CD. It should also include backup testing, documented recovery paths, dependency mapping, and release processes that account for restoration scenarios.
A modern engineering partner can help shorten that path when internal teams are stretched across compliance work, platform cleanup, and AI modernization. This kind of support matters most when leadership wants the product, infrastructure, and governance pieces to move together.
For organizations adding AI features, the roadmap also needs administrative controls around prompt and model operations. That includes versioned prompt management, parameter control for internal data access, centralized logging across integrated AI services, and visibility into cumulative model spend. Without those controls, AI adoption tends to outpace governance. In healthcare, that's a bad bargain.
Building the Future of Resilient Healthcare
The strongest case for DevOps in healthcare isn't that it helps teams ship faster. It's that it gives hospitals, healthtech vendors, and digital care platforms a safer way to change important systems. That includes clinician tools, patient experiences, integrations, and AI-powered workflows.
Done well, DevOps creates a delivery environment where compliance is more enforceable, security is less reactive, and operations are easier to trust. It reduces the hidden tax of manual releases, undocumented infrastructure, and last-minute security negotiations. It also gives leadership a better answer to a question that keeps getting harder: how do we modernize without increasing operational risk?
AI makes that question more urgent. As healthcare organizations add model-driven features and more dynamic data flows, release discipline becomes governance discipline. The teams that succeed won't be the ones with the flashiest demos. They'll be the ones that can prove what changed, protect sensitive data, recover cleanly, and keep critical services available.
DevOps is the foundation for that future. Not as a slogan. As a working system.
If you're rethinking how your organization delivers secure digital health products, Wonderment Apps can help you turn that strategy into an execution plan. Their team works across AI modernization, web and mobile product delivery, and operational governance for complex software systems. If you're exploring how to manage prompts, integrations, logging, parameter access, and AI cost visibility inside an existing application, it's worth booking a demo and seeing how their prompt management toolkit fits into a compliant healthcare roadmap.